
38 year old male was admitted hospital two month history fatigue and two week
A 38 year old male was admitted to hospital with a two month history of fatigue and a two week history of increasing edema. Congestive heart failure was diagnosed, and a cardiac catheterization revealed normal coronary arteries, but marked cardiac enlargement with four chamber dilation and mural thrombosis of the left ventricle. The cardiac index was 1.4. Further history revealed that he had been drinking a case of beer a day for many years and that he smoked one pack of cigarettes per day.
His condition acutely deteriorated two weeks later, with development of Enterobacter cloacae septicemia. He was transferred from a community hospital to a university hospital for management of sepsis and for possible cardiac transplantation. Despite antibiotic therapy and aggressive supportive measures, he expired the next day.
The following key laboratory findings were noted:
|
irosis |
PATIENT |
NORMAL RANGE |
|
WBC count |
9.4 K / microliter |
(3.7 – 9.9 K/microliter) |
|
Platelet count |
70 K / microliter |
(140 – 440 K/microliter) |
|
Hematocrit |
42% |
(44 – 50%) |
|
AST |
202 U/L |
(10 – 34 U/L) |
|
ALT |
139 U/L |
(6 – 59 U/L) |
|
GGTP |
124 U/L |
(0 – 51 U/L) |
|
LDH |
1218 U/L |
(105 – 230 U/L) |
|
Alk. Phos. |
119 U/L |
(45 – 150 U/L) |
|
Ammonia |
108 micromol/L |
(7 – 27 micromol/L) |
|
Total Protein |
7.9 G/dL |
(6.3 – 7.9 G/dL) |
|
Albumin |
3.6 G/dL |
(3.9 – 5.0 G/dL) |
|
Total bilirubin |
1.3 mg/dL |
(0.3 – 1.9 mg/dL) |
|
Direct bilirubin |
0.6 mg/dL |
( 0 – 0.3 mg/dL) |
|
Ferritin |
11,000 ng/mL |
(15 – 200 ng/mL) |
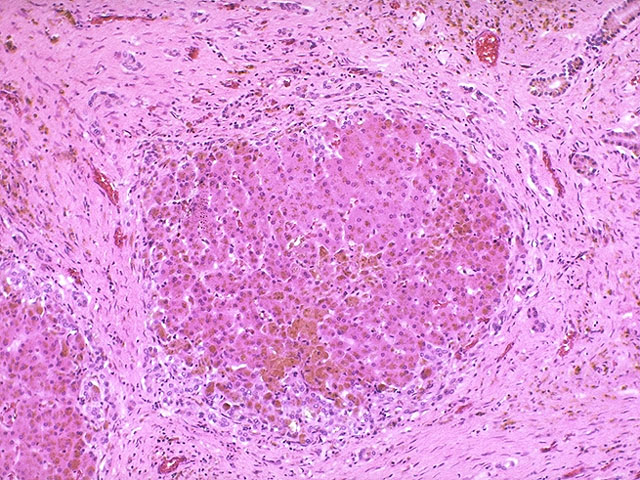
At autopsy, the liver weighed 2850 gm and had a finely nodular appearance. Sectioning revealed a firm, nodular cut surface. The liver, pancreas and lymph nodes all had a distinctly dark brown appearance on sectioning. The spleen weighed 530 gm. The heart weighed 650 gm and had four-chamber dilation. Coronary arteries showed no apparent atherosclerosis. The myocardium was dark brown and firm. The lungs were heavy (2000 gm total) and congested. There was a 1500 cc pleural effusion on the right and a 500 cc effusion on the left. There was 600 cc of ascitic fluid.
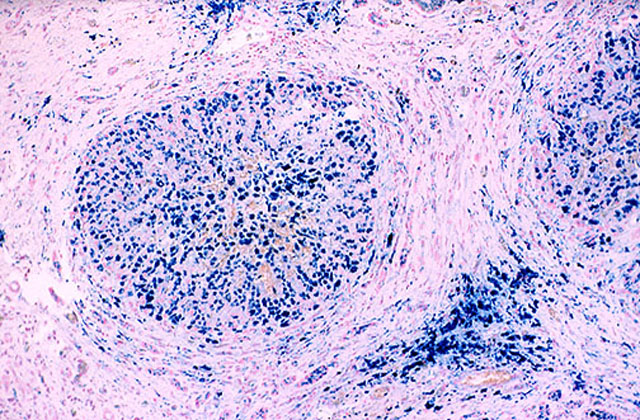
Microscopically the liver had extensive fibrosis with small nodules of hepatocytes without fatty change. There was the presence of abundant hemosiderin granules. There was no evidence of ischemic changes, but there was diffuse intersitital fibrosis, and iron stained myocardium also demonstrated extensive deposition of hemosiderin in and between myocardial fibers. Additional sites of extensive iron deposition included pancreas, lymph nodes, bone marrow, adrenals, pituitary, testes, thyroid, prostate, trachea, and brain.
1. Discuss the key laboratory findings in this case by relating the patient’s abnormal values to the pathogenesis of the disorder.
2. Describe the effect of the hemosiderin granules on the liver and heart and discuss the adaptive or non-adaptive response of both the liver and heart to the granular accumulation in this case.
3. Discuss the physiological events were responsible for the pleural effusion and ascites?
Do you need a similar assignment done for you from scratch? We have qualified writers to help you. We assure you an A+ quality paper that is free from plagiarism. Order now for an Amazing Discount!
Use Discount Code "Newclient" for a 15% Discount!
NB: We do not resell papers. Upon ordering, we do an original paper exclusively for you.


{kind=link}
{kind=link}
{kind=link}
{kind=link}